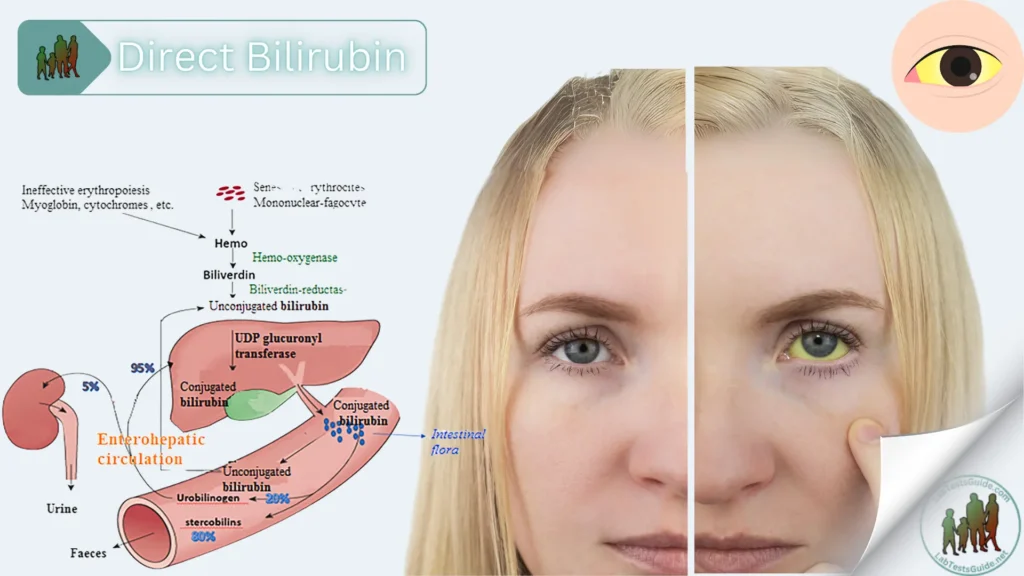
Indirect bilirubin is formed by the breakdown of hemoglobin in the red blood cells. The liver converts this bilirubin into direct bilirubin, which can then be released into the intestine by the gallbladder for elimination. Total bilirubin levels are therefore indicative of both the destruction of red blood cells and the proper functioning of the liver, gallbladder, and bile ducts.
Higher than normal levels of bilirubin may indicate different types of liver problems. Occasionally, higher bilirubin levels may indicate an increased rate of destruction of red blood cells (hemolysis).
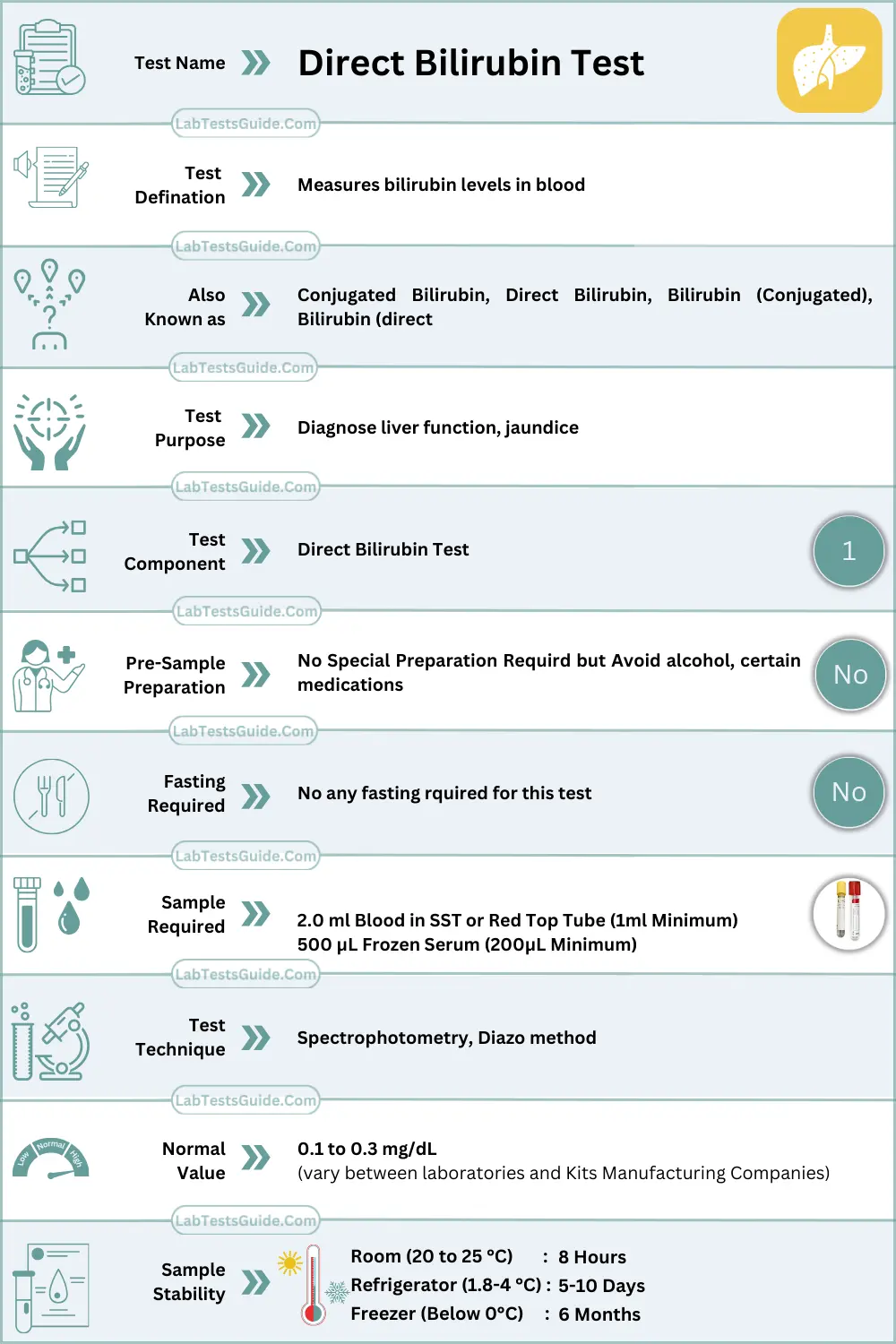
Also Known As: Total Bilirubin, TBIL, Neonatal Bilirubin, Direct Bilirubin, Conjugated Bilirubin, Indirect Bilirubin, Unconjugated Bilirubin, TB
Test Panel: Total Bilirubin, Conjagated Bilirubin, Unconjugated Bilirubin, ALT, AST, ALP, Total Protein, Albumin, Globulin, A/G ratio, GGT,
Why Get Tested :
- or the diagnosis of jaundice.
- To differentiate different types of jaundice.
- For the follow-up of a patient with treatment.
- To assess the progress of the disease.
- This test is done to evaluate the liver functions.
- This is done in a patient with hemolytic anemia in adults.
- It is also done to evaluate the hemolytic anemia in the newborn.
When to Get Tested:
Your doctor may order a bilirubin test if you:
- Show signs of jaundice
- Have anemia, or low red blood cells
- Might be having a toxic reaction to drugs
- Have a history of heavy drinking
- Have been exposed to hepatitis viruses
- Have cirrhosis
You might also have your bilirubin tested if you have symptoms like:
- Dark urine
- Nausea and vomiting
- Abdominal pain or abdominal swelling
- Clay-colored stools
- Fatigue
When Bilirubin Test Ordered:
A health practitioner usually orders a bilirubin test in conjunction with other laboratory tests (alkaline phosphatase, AST, ALT) when someone shows signs of abnormal liver function. A bilirubin level may be ordered when a person:
- Shows evidence of jaundice
- Has a history of drinking excessive amounts of alcohol
- Has suspected drug toxicity
- Has been exposed to hepatitis-causing viruses
Other symptoms that may be present include:
- Dark, amber-colored urine
- Nausea/vomiting
- Abdominal pain and/or swelling
- Fatigue and general malaise that often accompany chronic liver disease
Measuring and monitoring bilirubin in newborns with jaundice is considered standard medical care.
Tests for bilirubin may also be ordered when someone is suspected of having (or known to have) hemolytic anemia as a cause of anemia. In this case, it is often ordered along with other tests used to evaluate hemolysis, such as complete blood count, reticulocyte count, haptoglobin, and LDH.
- Raised Bilirubin is the indicator of liver dysfunction.
- Bilirubin is the basic end product of Hemoglobin metabolism.
- Total Bilirubin (Direct Bilirubin + Indirect Bilirubin)
- Direct Bilirubin (Conjugated Bilirubin)
- Indirect Bilirubin (Unconjugated Bilirubin)
Sample Required
- This test is done in the serum of the patient.
- The random sample can be taken and no need for a fasting sample.
- From infants, the blood may be collected from the heel.
- The sample is stable at 4 °C for 3 days and protects it from the light.
Precautions for Sample :
- Avoid hemolysis.
- Avoid shaking of the tube that may lead to inaccurate results.
- Do not expose the tube to light. Exposure to light like the sun or even artificial light may decrease the value.
- If there is a delay in the test then keep the sample away from the light and refrigerate it.
Normal Values:
- Total bilirubin = 0.3 to1.0 mg/dL or 5.1 to 17.0 mmol/L
- Direct bilirubin = 0.1 to 0.3 mg/dL or 1.0 to 5.1 mmol/L
- Indirect bilirubin (total bilirubin – direct bilirubin level) = 0.2–0.7 mg/dL
Raised level of direct bilirubin is seen in:
- Gallstones.
- Gallbladder tumors.
- Inflammatory scarring or obstruction of extrahepatic ducts.
- Extensive liver metastasis.
- Dubin-Johnson syndrome.
- Rotor syndrome.
- Drugs may cause cholestasis.
- Please see more details on bilirubin Total
Table showing the Different type of Jaundice and their causes
| Type of Jaundice | Causes | Pathophysiology |
| Unconjugated hyperbilirubinemia | Extravascular hemolysis | Heme is converted to unconjugated bilirubin |
| Right heart failure and Cirrhosis | There is a defect in the delivery of unconjugated bilirubin to liver | |
| Hypothyroidism and Crigler-Najjar syndrome | There is a defect in the conjugation of bilirubin in the hepatocytes | |
| Drugs like Rifampicin and Gilbert syndrome | There is a defect in the uptake of unconjugated bilirubin into hepatocytes | |
| Conjugated hyperbilirubinemia | Mechanical obstruction by tumors, stones or strictures, and primary biliary cirrhosis | There is a defect in the flow of conjugated bilirubin through canaliculi and bile ducts. Called cholestatic jaundice. |
| Drugs like estrogen and cyclosporineDubin-Johnson syndromePregnancy | There is a defect in the transmembrane secretion of conjugated bilirubin into the canaliculus. This is also called hepatocellular jaundice | |
| Sepsis | Like above |