AFB Smear and Culture Test – Accurate Detection of Tuberculosis & Acid-Fast Bacteria
An AFB (acid-fast bacilli) smear and culture test detects mycobacteria, primarily Mycobacterium tuberculosis (which causes tuberculosis), by looking for these bacteria in body fluids or tissues (such as sputum) using a special stain and microscopic examination (smear), followed by culturing the bacteria in a laboratory (culture) for definitive identification and susceptibility testing; the smear provides rapid but nonspecific results and the culture provides confirmation for several weeks.

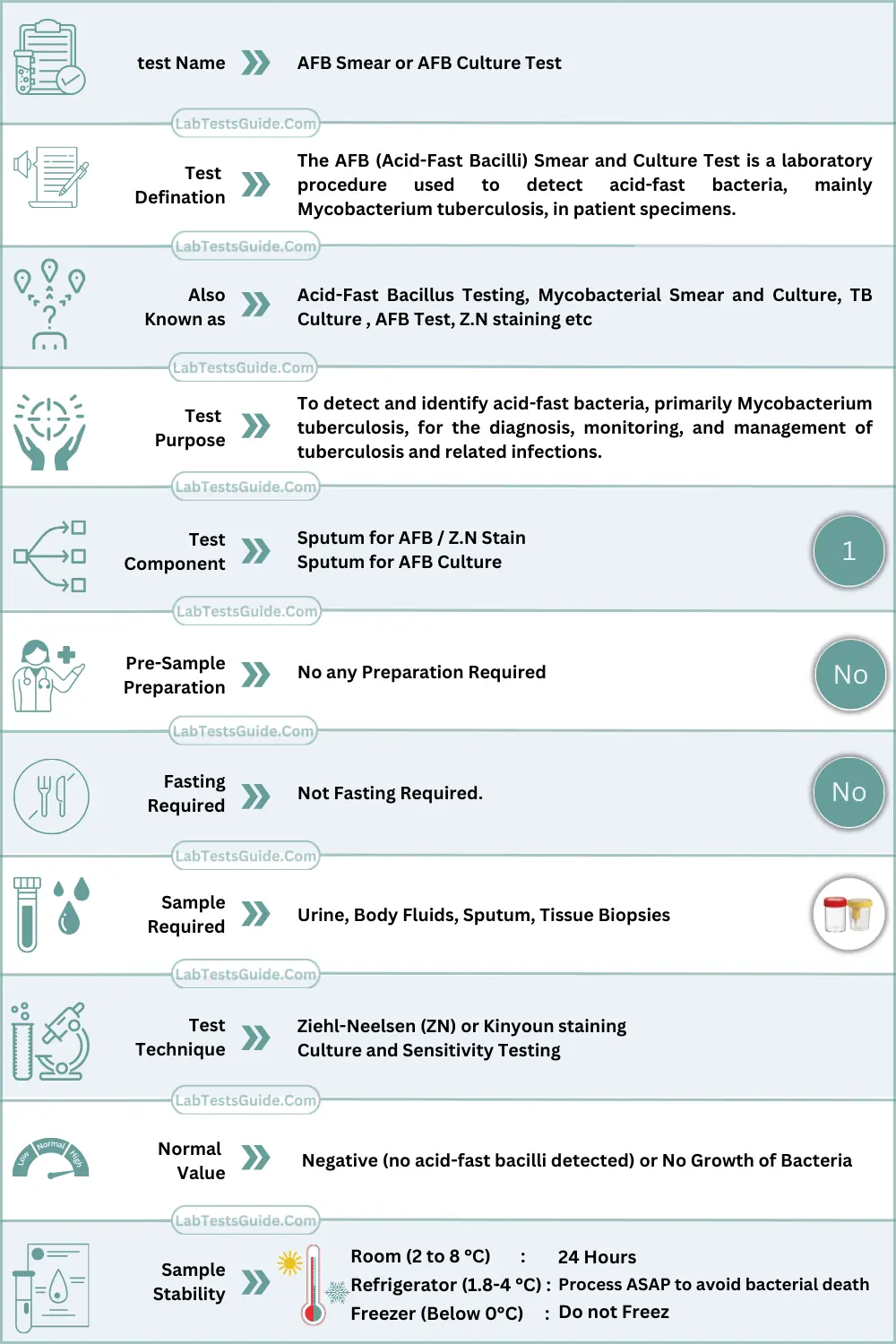
AFB Smear and SFB Culture Test Quick Facts Table:
What is AFB Smear and Culture Test ?
The AFB (Acid-Fast Bacilli) Smear and Culture Test is a laboratory procedure used to detect acid-fast bacteria, mainly Mycobacterium tuberculosis, in patient specimens. It helps diagnose tuberculosis and related infections by visually identifying bacteria under a microscope and by growing them in culture.
Why is AFB Smear and Culture Test Done ?
For Patients / General Use
- Persistent cough lasting >2–3 weeks
- Fever, night sweats, weight loss
- Coughing up blood (hemoptysis)
- Suspected exposure to tuberculosis
- Monitoring response to TB treatment
For Doctors / Clinical Use
- Confirm or rule out tuberculosis
- Identify non-tuberculous mycobacterial infections
- Guide antibiotic selection based on culture and sensitivity
- Monitor treatment efficacy in known TB patients
How the AFB Smear and Culture Test Works (Principle / Methodology):
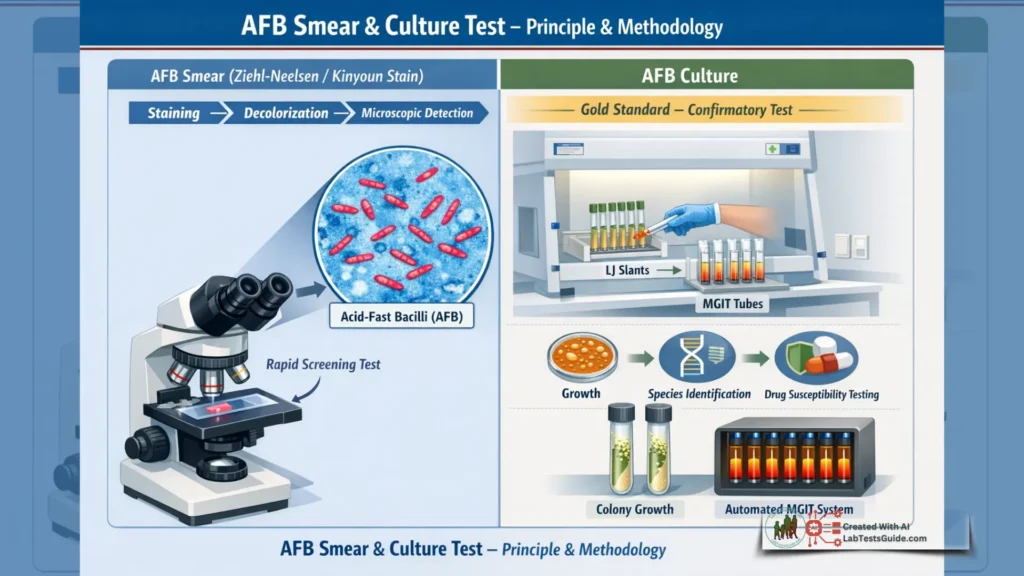
- AFB Smear: Uses Ziehl-Neelsen or Kinyoun staining to detect acid-fast bacilli in specimens. Acid-fast bacteria retain red dye (carbol fuchsin) despite acid-alcohol decolorization, allowing microscopic identification.
- AFB Culture: Specimens are inoculated onto Lowenstein-Jensen (solid) or liquid media (e.g., MGIT) to grow mycobacteria. Cultures allow definitive identification, differentiation of species, and drug susceptibility testing.
AFB Smear and Culture Test Specimen Requirements & Collection
| Parameter | Details |
|---|---|
| Specimen type | Sputum (preferred), BAL, tissue biopsy, body fluids |
| Tube type | Sterile, leak-proof container |
| Volume | 2–5 mL for sputum; 1–2 mL for fluids/tissues |
| Patient preparation | Early morning sputum recommended; rinse mouth with water prior to collection |
| Collection steps | – Deep cough specimen into container – Avoid saliva only samples – Label with patient info, date, and time |
| Transport & storage | Room temperature if <24 h; refrigerate at 2–8°C if longer; process ASAP to avoid bacterial death |
AFB Smear and Culture Test Reference Ranges
| Population | Reference Range | Units |
|---|---|---|
| All adults & children | Negative (no AFB detected) | N/A |
| Pregnant patients | Negative | N/A |
| Note | Positive results indicate infection; ranges may vary by lab and method | N/A |
AFB Smear and Culture Test Interpretation of Results:
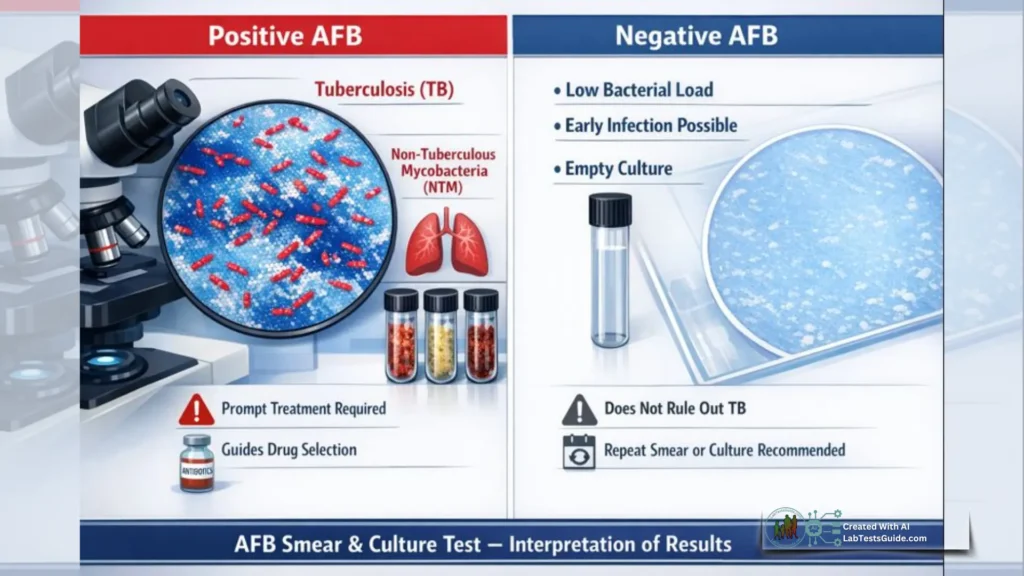
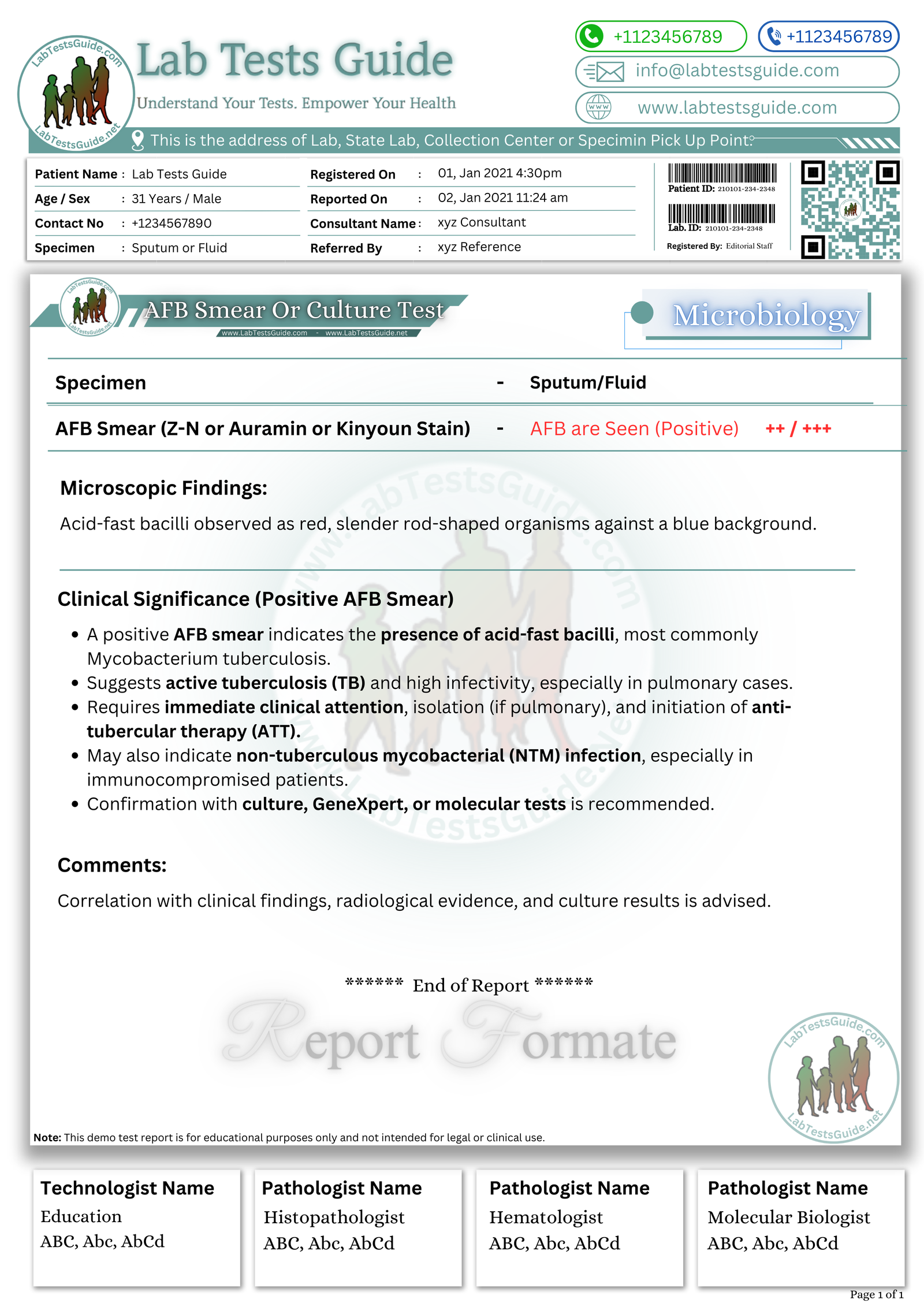
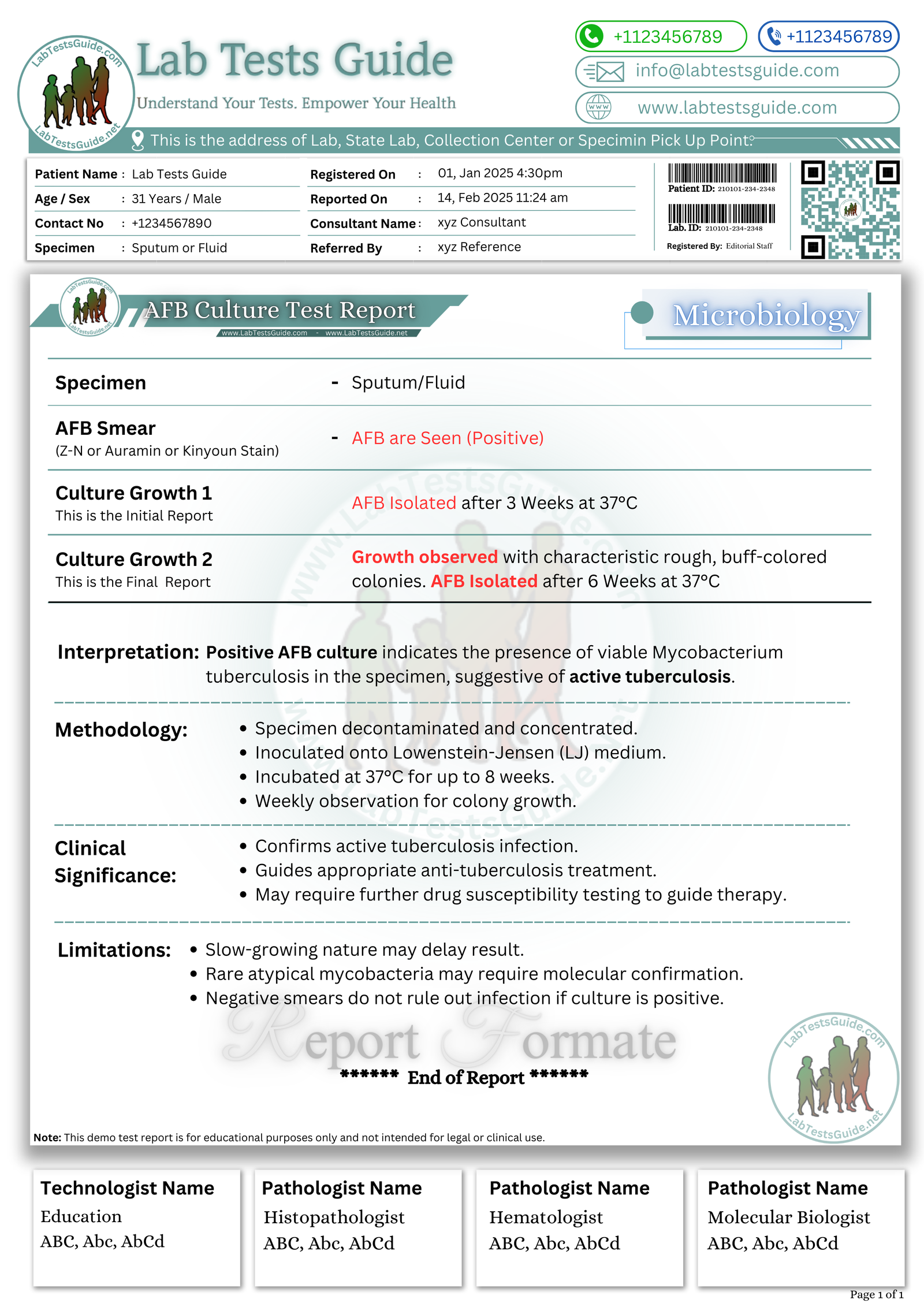
High Levels (Positive AFB)
- Causes: Tuberculosis, non-tuberculous mycobacterial infection, lab contamination
- Differential diagnoses: Pulmonary TB, extrapulmonary TB, atypical mycobacterial infection
- Clinical relevance: Requires prompt treatment initiation; guides antibiotic choice
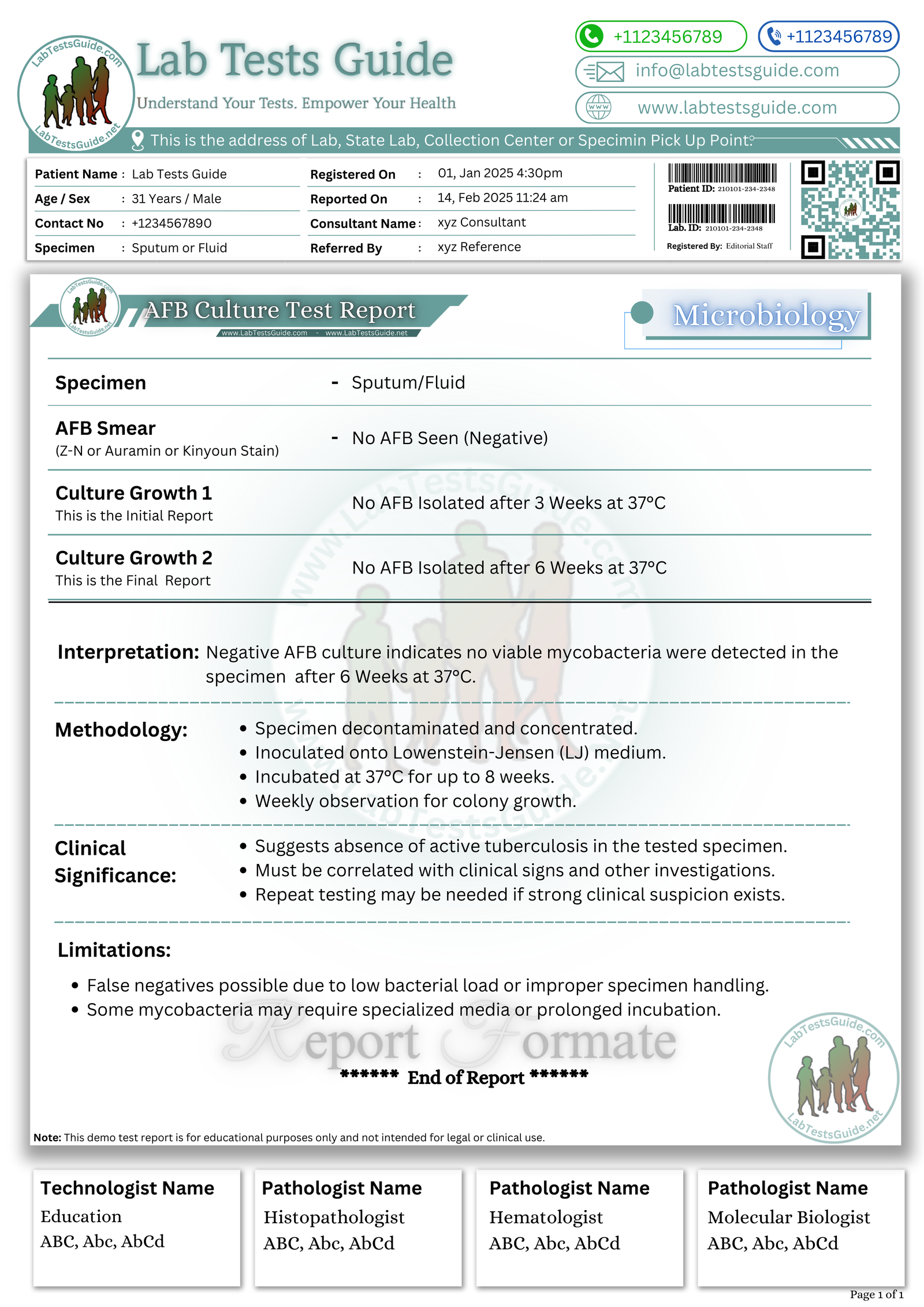
Low Levels (Negative AFB)
- Causes: No infection, early disease, inadequate specimen
- Differential diagnoses: False negatives due to low bacterial load
- Clinical relevance: Does not completely rule out TB; repeat testing or culture may be needed
Interfering Factors / Pre-Analytical Errors
- Hemolysis effect: Minimal for smear, can affect culture viability if severe
- Medications: Antibiotics may reduce bacterial load
- Sample handling issues: Delay in transport can reduce bacterial viability
- Biological variations: Early infection may yield false negatives
Critical Values / PANIC Values
- Positive AFB smear or culture: Considered critical; immediate clinical notification required
- Note: Follow institutional policy for urgent reporting
🧠 AI-Powered Test Result Analysis:
Understand your AFB Smear and Culture Test – Accurate Detection of Tuberculosis & Acid-Fast Bacteria Results
AI-powered Lab Test Results Meaning tool 🤖
📥 Download AFB Smear and Culture Lab Report Format
Get the demo report format for AFB Smear and Culture in your preferred format. These templates are fully editable and professional.
How to Download?
| File Description | Format |
|---|---|
AFB Smearm Test (Negative) Report Format (Image) | .PNG |
AFB Smearm Test (Negative) Report Format (MS Word) | .DOCX |
AFB Smearm Test (Negative) Report Format (MS Excel) | .XLSX |
AFB Smearm Test (Negative) Report Format (PDF) |
{kind=link}
| File Description | Format |
|---|---|
AFB Smearm Test (Positive) Report Format (Image) | .PNG |
AFB Smearm Test (Positive) Report Format (MS Word) | .DOCX |
AFB Smearm Test (Positive) Report Format (MS Excel) | .XLSX |
AFB Smearm Test (Positive) Report Format (PDF) |
{kind=link}
| File Description | Format |
|---|---|
AFB Culture Test (Negative) Report Format (Image) | .PNG |
AFB Culture Test (Negative) Report Format (MS Word) | .DOCX |
AFB Culture Test (Negative) Report Format (MS Excel) | .XLSX |
AFB Culture Test (Negative) Report Format (PDF) |
{kind=link}
| File Description | Format |
|---|---|
AFB Culture Test (Positive) Report Format (Image) | .PNG |
AFB Culture Test (Positive) Report Format (MS Word) | .DOCX |
AFB Culture Test (Positive) Report Format (MS Excel) | .XLSX |
AFB Culture Test (Positive) Report Format (PDF) |
{kind=link}
AFB Lab Reports (Demo Reports Format):
Nursing / Phlebotomy Notes
- Use sterile, leak-proof container (no additives)
- Label with patient name, ID, date, and time
- Transport promptly; refrigerate if delayed >24 h
- Avoid contamination with saliva
- Follow biosafety precautions for infectious specimens
Lab Student Key Points
- Smear provides rapid but less sensitive detection
- Culture is gold standard; slower but more definitive
- Early morning sputum improves yield
- Negative smear does not rule out TB
How long does it take to get AFB culture results?
Typically 2–8 weeks, depending on medium.
Can a negative smear rule out TB?
No, culture may still detect bacteria.
Is fasting required for this test?
No
Can antibiotics affect results?
Yes, they can reduce bacterial detection.
What if the test is positive?
Your doctor will guide further management and treatment.
Can children have this test?
Yes, with appropriately collected sputum or other specimens
Is the test painful?
No, it is non-invasive for sputum; tissue collection may require a procedure.