Direct vs Indirect Bilirubin: The Clinical Comparison
An advanced laboratory guide to understanding conjugated and unconjugated bilirubin metabolism, diagnostic significance, and clinical markers for jaundice.
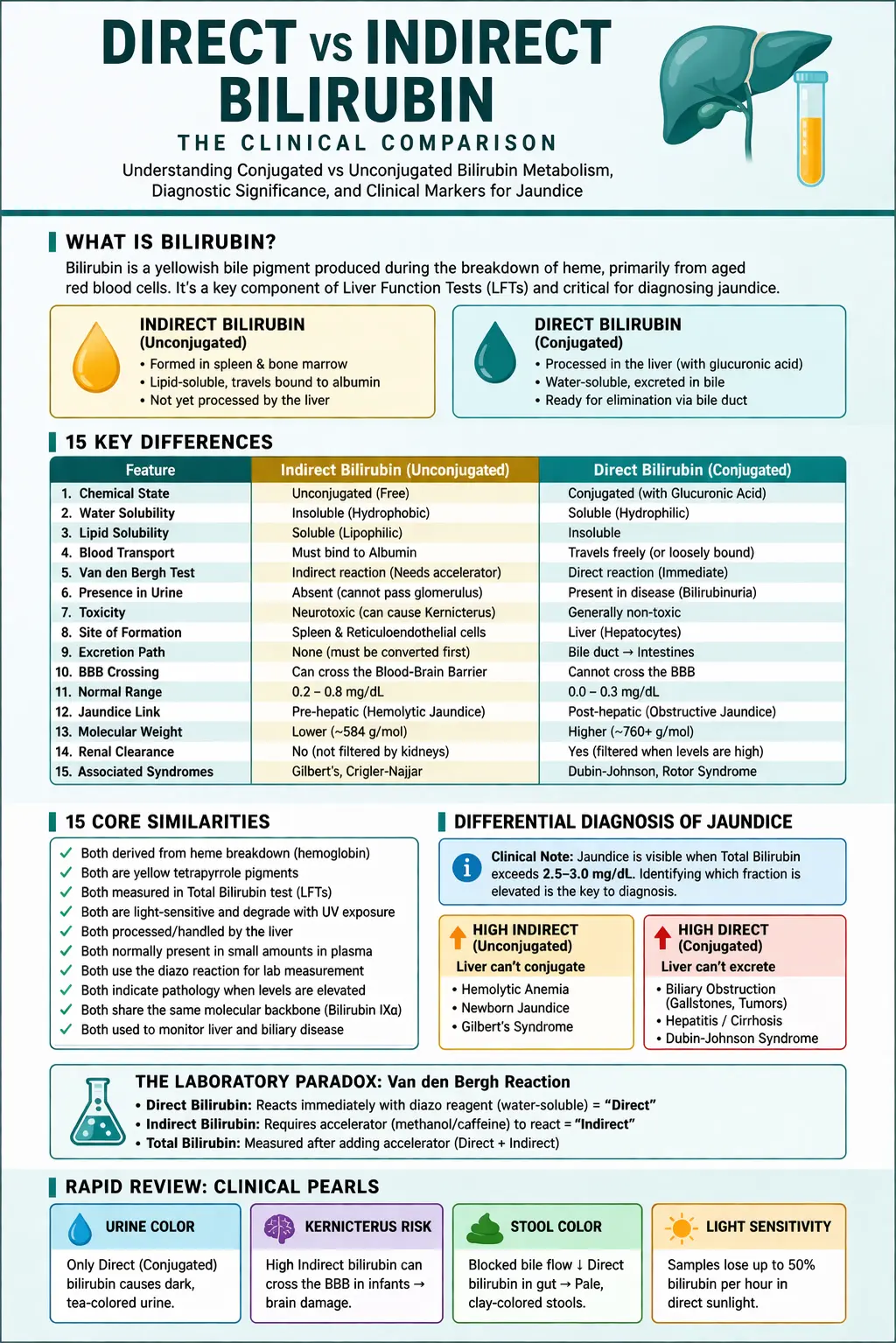
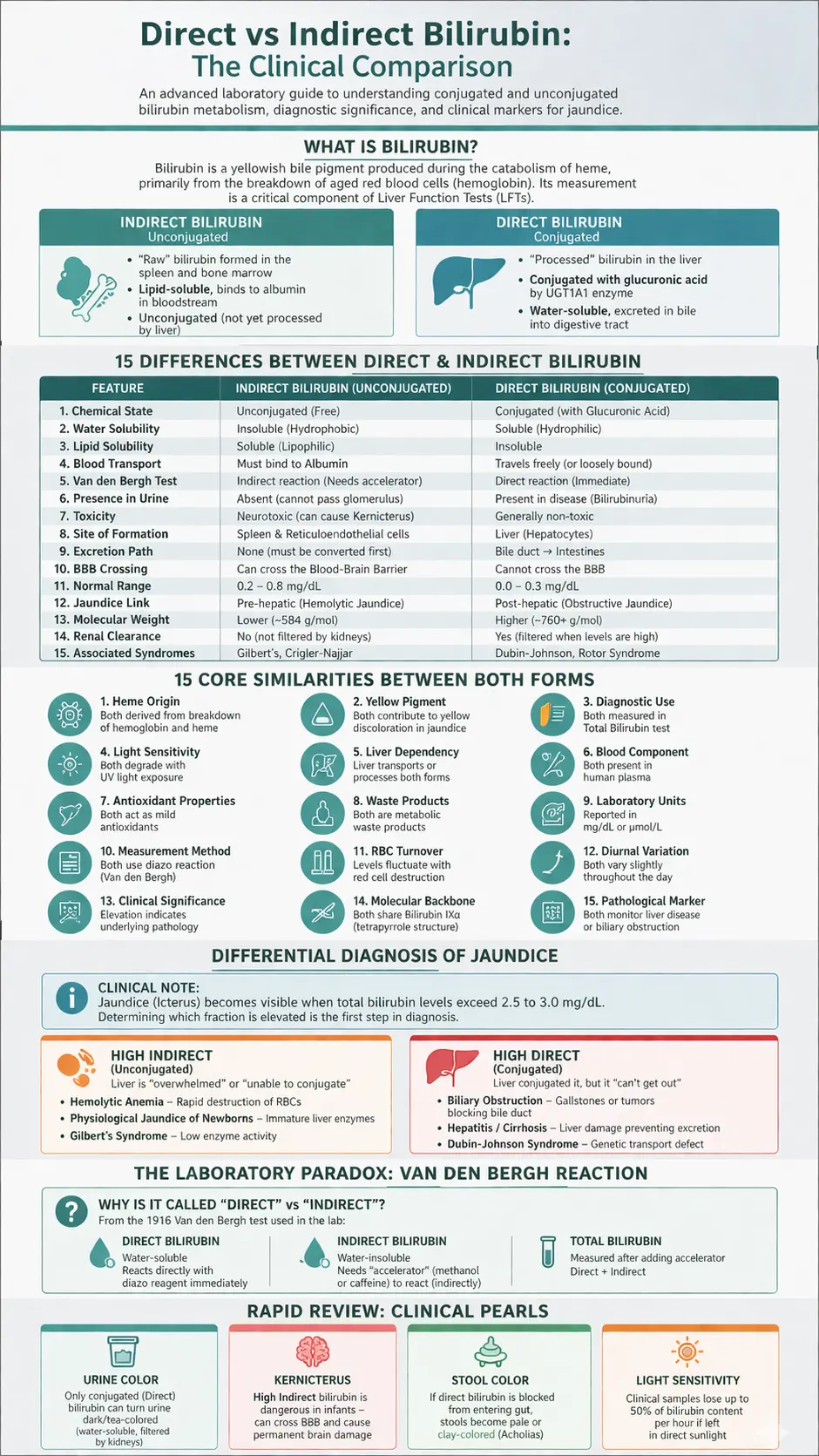
What is Bilirubin?
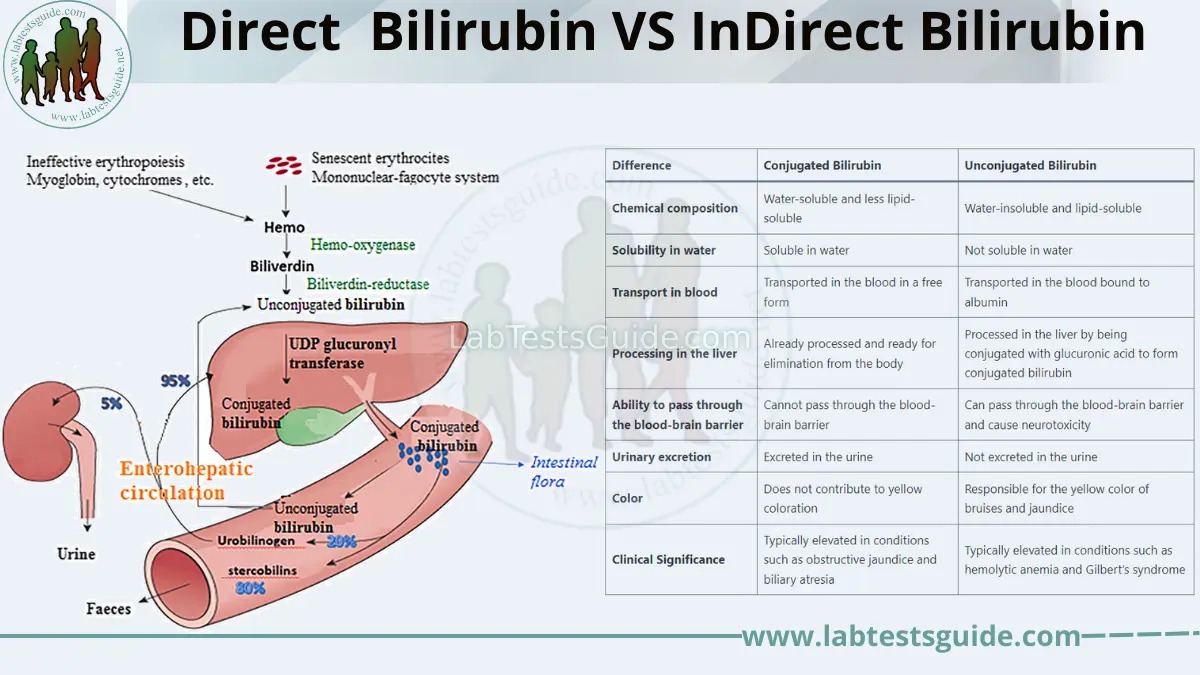
Bilirubin is a yellowish bile pigment produced during the catabolism of heme, primarily from the breakdown of aged red blood cells (hemoglobin). Its measurement is a critical component of Liver Function Tests (LFTs).
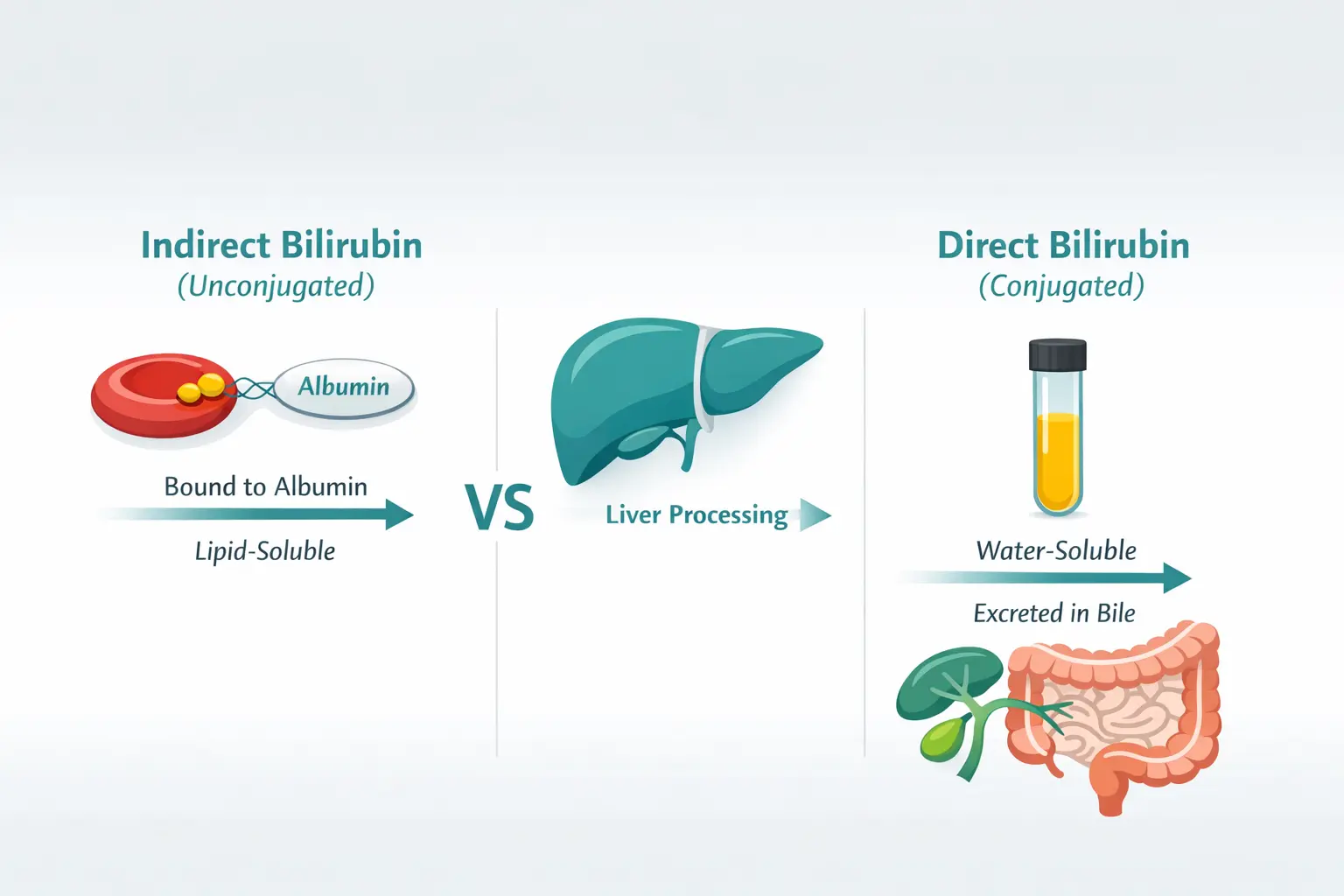
Direct Bilirubin (Conjugated)
This is the “processed” bilirubin. The liver attaches glucuronic acid to indirect bilirubin using the enzyme UGT1A1, making it water-soluble. This allows it to be excreted into the bile and eventually the digestive tract.

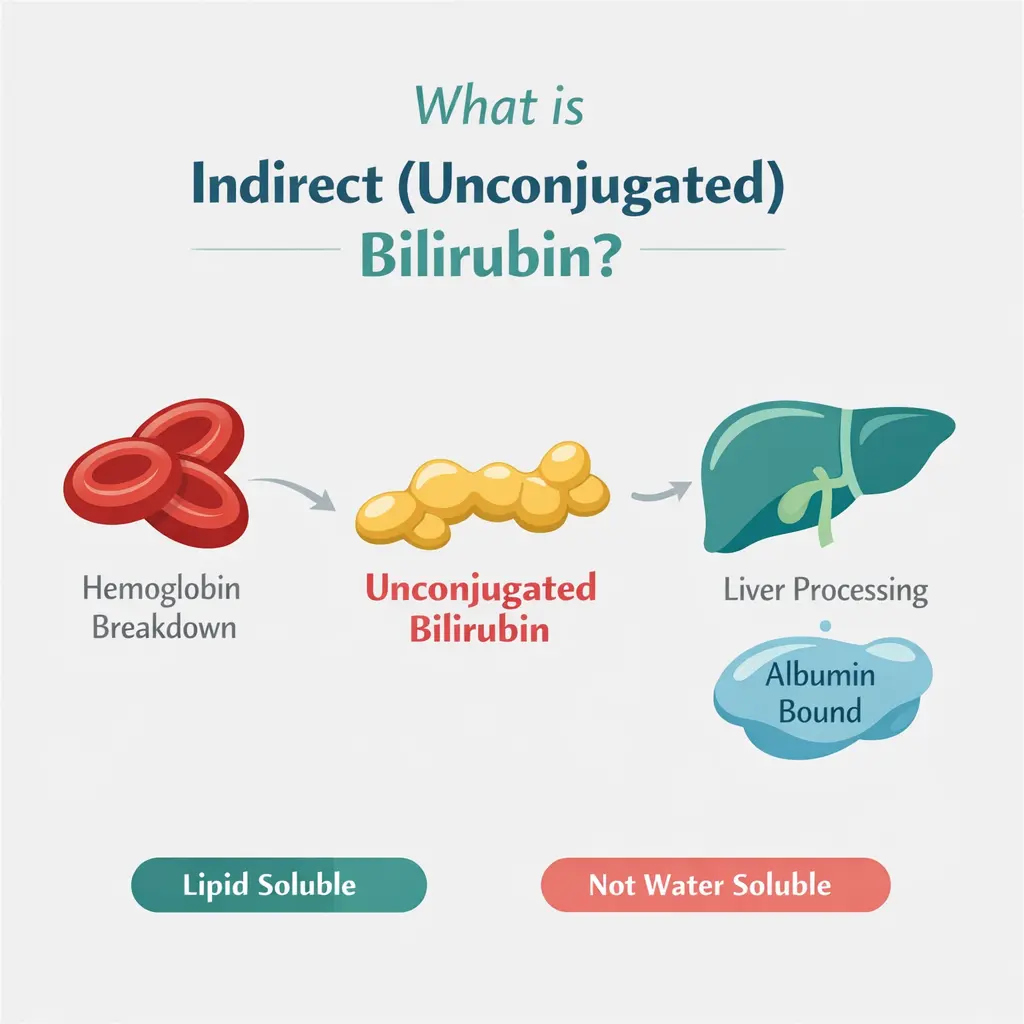
Indirect Bilirubin (Unconjugated)
This is the “raw” bilirubin formed in reticuloendothelial system (RES) (mainly spleen, liver, bone marrow). It is lipid-soluble and travels through the bloodstream bound to albumin. Because it hasn’t been processed by the liver yet, it is “unconjugated.”
15 Differences Between Direct & Indirect Bilirubin
| Feature | Indirect Bilirubin (Unconjugated) | Direct Bilirubin (Conjugated) |
|---|---|---|
| 1. Chemical State | Unconjugated (Free) | Conjugated (with Glucuronic Acid) |
| 2. Water Solubility | Insoluble (Hydrophobic) | Soluble (Hydrophilic) |
| 3. Lipid Solubility | Soluble (Lipophilic) | Insoluble |
| 4. Blood Transport | Must bind to Albumin | Travels freely (or loosely bound) |
| 5. Van den Bergh Test | Indirect reaction (Needs accelerator) | Direct reaction (Immediate) |
| 6. Presence in Urine | Absent (cannot pass glomerulus) | Present in disease (Bilirubinuria) |
| 7. Toxicity | Neurotoxic (can cause Kernicterus) | Generally non-toxic |
| 8. Site of Formation | Spleen & Reticuloendothelial cells | Liver (Hepatocytes) |
| 9. Excretion Path | None (must be converted first) | Bile duct → Intestines |
| 10. BBB Crossing | Can cross the Blood-Brain Barrier | Cannot cross the BBB |
| 11. Normal Range | 0.2 – 0.8 mg/dL | 0.0 – 0.3 mg/dL |
| 12. Jaundice Link | Pre-hepatic (Hemolytic Jaundice) | Post-hepatic (Obstructive Jaundice) |
| 13. Molecular Weight | Lower (~584 g/mol) | Higher (~760–800 g/mol) |
| 14. Renal Clearance | No (not filtered by kidneys) | Yes (filtered when levels are high) |
| 15. Associated Syndromes | Gilbert’s, Crigler-Najjar | Dubin-Johnson, Rotor Syndrome |
15 Core Similarities Between Both Forms
Differential Diagnosis of Jaundice
High Indirect (Unconjugated)
Suggests the liver is “overwhelmed” or “unable to conjugate”:
- Hemolytic Anemia: Rapid destruction of RBCs.
- Physiological Jaundice of Newborns: Immature liver enzymes.
- Gilbert’s Syndrome: Low enzyme activity.
High Direct (Conjugated)
Suggests the liver conjugated it, but it “can’t get out”:
- Biliary Obstruction: Gallstones or tumors blocking the bile duct.
- Hepatitis/Cirrhosis: Liver damage preventing excretion.
- Dubin-Johnson Syndrome: Genetic transport defect.
The Laboratory Paradox: Van den Bergh Reaction
Why is it called “Direct” vs “Indirect”?
The names come from the 1916 Van den Bergh test used in the lab:
- Direct Bilirubin: Being water-soluble, it reacts directly with the diazo reagent immediately upon mixing.
- Indirect Bilirubin: Being water-insoluble, it does not react until an “accelerator” (like methanol or caffeine) is added to the solution to make it accessible. It reacts indirectly.
- Total Bilirubin: The measurement taken after adding the accelerator (Direct + Indirect).
Rapid Review: Microbiology & Clinical Pearls
Urine Color
Only conjugated (Direct) bilirubin can turn urine dark/tea-colored because it is water-soluble and filtered by kidneys.
Kernicterus
High Indirect bilirubin is dangerous in infants because it can cross the BBB and cause permanent brain damage.
Stool Color
If direct bilirubin is blocked from entering the gut (obstruction), stools become pale or clay-colored (Acholias).
Light Sensitivity
Clinical samples lose up to 50% of bilirubin content per hour if left in direct sunlight.
FAQs:
What is bilirubin?
Bilirubin is a yellow pigment that is formed from the breakdown of red blood cells. It is processed by the liver and excreted in the bile.
What is Direct bilirubin?
Direct bilirubin is bilirubin that has been processed by the liver and is soluble in water. It is excreted in the bile and eventually eliminated from the body.
What is InDirect bilirubin?
InDirect bilirubin is bilirubin that has not been processed by the liver and is insoluble in water. It is bound to albumin and transported to the liver for processing.
What causes high levels of InDirect bilirubin?
High levels of InDirect bilirubin can be caused by hemolytic anemia, where red blood cells are destroyed faster than the liver can process bilirubin. Gilbert’s syndrome, a genetic disorder that affects the liver’s ability to process bilirubin, can also lead to elevated unconjugated bilirubin levels.
What causes high levels of Direct bilirubin?
High levels of Direct bilirubin can be caused by liver damage or obstruction of the bile ducts. This can occur in conditions such as hepatitis, cirrhosis, or biliary atresia.
What is the significance of bilirubin levels in newborns?
Elevated levels of InDirect bilirubin in newborns can lead to a condition called neonatal jaundice. This occurs when the newborn’s liver is not yet fully developed and is unable to process bilirubin efficiently. Phototherapy is often used to treat neonatal jaundice.
What is the difference between direct and indirect bilirubin?
Direct bilirubin refers to Direct bilirubin, while indirect bilirubin refers to InDirect bilirubin.
How are bilirubin levels measured?
Bilirubin levels are measured using a blood test, which can determine the levels of both conjugated and unconjugated bilirubin.
How are high bilirubin levels treated?
The treatment for high bilirubin levels depends on the underlying cause. Phototherapy is often used to treat neonatal jaundice. Liver disease may require medication or surgery.
What are the symptoms of high bilirubin levels?
Symptoms of high bilirubin levels can include yellowing of the skin and eyes (jaundice), itching, fatigue, and pale-colored stools.
Can high bilirubin levels be prevented?
Preventing high bilirubin levels depends on the underlying cause. Some liver diseases may be prevented by maintaining a healthy lifestyle, avoiding alcohol, and getting vaccinated for hepatitis.
Is bilirubin testing a routine part of medical exams?
Bilirubin testing is not a routine part of medical exams but may be ordered if a doctor suspects liver or blood disorders. It may also be part of newborn screening tests.