Understanding Curcumin Bioavailability: Why Delivery Systems Matter for Inflammatory Biomarkers and Lab Results
Turmeric (Curcuma longa) has transitioned from traditional medicine into a cornerstone of functional healthcare. Its primary active polyphenol, curcumin, is widely recognized for its profound ability to modulate inflammatory pathways, neutralize systemic oxidative stress, and balance metabolic health markers.
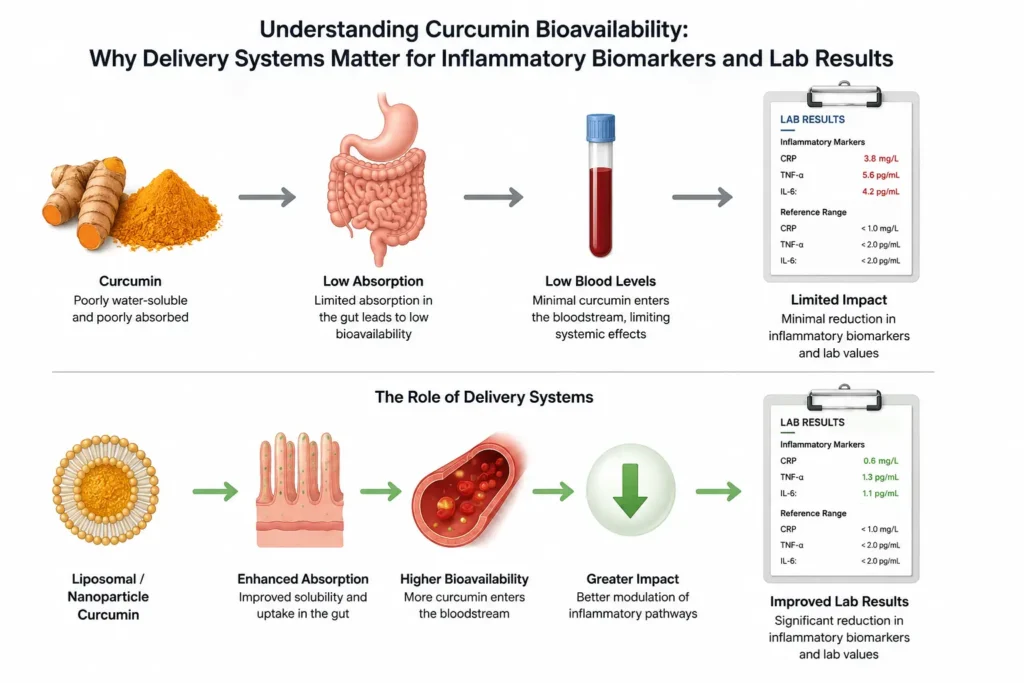
However, patients tracking their health via routine blood tests frequently hit a frustrating wall: they take high-dose turmeric supplements every day, yet their systemic inflammatory markers—like C-Reactive Protein (CRP) or Erythrocyte Sedimentation Rate (ESR)—remain stubbornly unchanged.
This diagnostic discrepancy highlights the “curcumin conundrum.” In vitro (test tube) studies show extraordinary biochemical potency, but in vivo (inside the human body), native curcumin possesses an incredibly poor pharmacokinetic profile. For readers analyzing their blood work, understanding curcumin bioavailability—the rate and extent to which an active compound enters systemic circulation—is crucial to achieving measurable clinical outcomes.
The Biological Reality: Why Standard 95% Extract Fails to Absorb
The market is saturated with supplements claiming maximum potency because they contain “Standardized 95% Curcuminoids.” While chemically pure, this crystalline powder is structurally ill-equipped to handle the human digestive tract. Native curcumin faces four distinct physiological barriers that severely limit its clinical efficacy:
- Hydrophobicity and Poor Aqueous Solubility: Curcumin is lipophilic (fat-loving) and highly hydrophobic (water-fearing). Because your gastrointestinal tract is an entirely aqueous environment, standard raw powder cannot dissolve efficiently. Instead, it clumps together, passes through the digestive tract unabsorbed, and is rapidly excreted.
- Low Epithelial Permeability: Even the small fraction of curcumin that manage to dissolve struggles to cross the intestinal barrier. Its native molecular structure prevents efficient passive diffusion across the epithelial cell membranes of the small intestine.
- Rapid First-Pass Metabolism (Phase-II Conjugation): Your liver and intestines treat free curcumin as a foreign compound that must be cleared immediately. Enzymes quickly attach sugar or sulfur molecules to it, converting it into inactive metabolites like curcumin glucuronide and curcumin sulfate.
- Rapid Elimination: Once metabolized into these water-soluble forms, the compound is flushed out of the body through bile and kidneys within hours, resulting in negligible steady-state plasma concentrations.
Because of these compounding hurdles, human clinical trials show that taking up to 10 grams of standard unformulated curcumin yields barely detectable or completely sub-therapeutic serum levels in laboratory blood tests.
Advanced Delivery Systems vs. Standard Extracts
To transform curcumin from a poorly absorbed botanical into a highly systemic therapeutic tool, modern nutritional science has shifted away from simply raising the milligram dosage. Instead, the focus is entirely on altering the physical and chemical delivery matrix to protect the fragile molecule and enhance intestinal uptake.
1. The Adjuvant Approach: Piperine Co-Administration
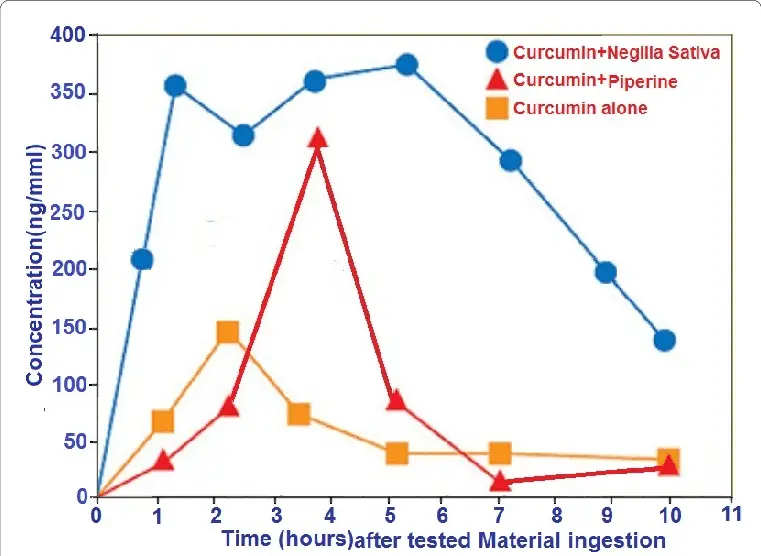
One of the earliest methods developed to bypass rapid hepatic metabolism is combining curcumin with piperine, the sharp alkaloid found in black pepper. Piperine acts as a non-specific inhibitor of UDP-glucuronosyltransferase—the precise liver and bowel enzyme responsible for glucuronidation.
By temporarily putting these metabolic clearance pathways on hold, piperine allows free curcumin to enter the bloodstream intact. Clinical studies demonstrate that co-administering 20 mg of piperine can boost relative bioavailability by up to 2,000% (a 20-fold increase).
Diagnostic Note: While a 2,000% relative increase sounds massive, it starts from a baseline of nearly zero. Furthermore, because piperine is a non-specific enzyme inhibitor, it can alter the clearance rates of prescription medications, making it a less ideal option for individuals on complex pharmaceutical protocols.
2. Phospholipid Complexes (Phytosomes)
Rather than blocking liver enzymes, phytosome technology alters how the molecule interacts with liquid environments. Individual curcumin molecules are chemically bound to a phospholipid core (such as phosphatidylcholine derived from non-GMO sunflower lecithin). Because phospholipids have an amphiphilic nature—meaning they possess a water-soluble head and a fat-soluble tail—they create a molecular bridge. This allows the compound to dissolve seamlessly in gastric fluids and slip easily past the lipophilic intestinal walls.
3. Liposomal Encapsulation
Representing the pinnacle of targeted lipid-based delivery, a liposome is a microscopic, spherical vesicle composed of a phospholipid bilayer surrounding an aqueous core. This structure perfectly mimics the architecture of human living cell membranes.
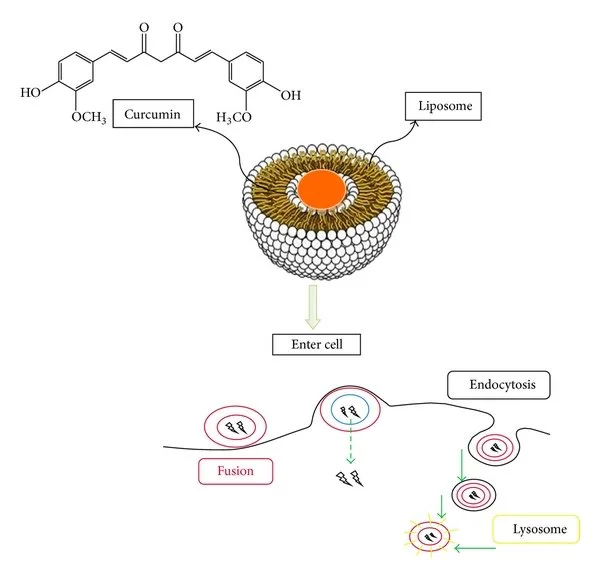
During advanced manufacturing, hydrophobic curcumin molecules are securely locked directly inside the protective lipid bilayer sheets. This structural shield prevents the fragile polyphenol from being degraded by harsh stomach acids and digestive enzymes.
When the liposomal sphere reaches the small intestine, it completely bypasses traditional, slow transporter pathways. Instead, the liposome can fuse directly with the lipid membranes of the intestinal cells, entering systemic circulation intact. For individuals searching for stable ingredients for clean formulations, exploring commercial raw materials optimized for liposomal encapsulation offers a highly protective, premium delivery standard.
4. Nanoparticles and Micellar Systems
Nanotechnology tackles the absorption bottleneck by shrinking particle sizes down to a sub-microscopic scale (typically 10 to 100 nanometers). Engineering curcumin into solid lipid nanoparticles exponentially increases its surface-area-to-volume ratio. These ultra-small particles disperse perfectly in water without clumping, enabling them to easily navigate the mucosal layers of the gut with minimal biological resistance.
Comparing the Bioavailability Spectrum
| Delivery Formulation | Primary Absorption Mechanism | Relative Bioavailability Factor | Clinical Target Area |
| Standard Curcumin 95% Extract | Native crystalline powder; relies entirely on raw digestive capacity. | 1x (Baseline / Less than 1% absorption) | Localized GI tract (e.g., colon health, IBS) |
| Curcumin + Piperine (Black Pepper) | Intestinal and hepatic enzyme inhibition; blocks glucuronidation. | ~20x (Highly variable) | Mild systemic issues; localized joint support |
| Phytosome (Phospholipid Complex) | Lipid complexation; improves membrane transport and compatibility. | ~29x to 30x | Systemic inflammation, joint, and vascular health |
| Liposomal Encapsulation | Spherical lipid bilayers; shields compound for direct membrane fusion. | Significant Systemic Elevation | Advanced therapeutic protocols; systemic neuroprotective support |
| Nanoparticles / Micelles | Sub-micron surface reduction; extreme water dispersion. | 57x to 100x+ | High-potency systemic tissue saturation |
Clinical Implications: Connecting Supplement Form to Lab Biomarkers
In clinical pharmacology and laboratory analytics, blood serum concentrations dictate real-world outcomes. If a natural compound cannot achieve a high enough steady-state plasma concentration, it will fail to activate cellular receptors or downregulate systemic inflammatory genes.
When selecting a formula to manage or improve specific lab markers, the target location dictates the delivery system you need:
- For Localized GI Issues: If you are using turmeric solely to address conditions within the digestive tract, such as inflammatory bowel issues or localized gut irritation, a cheap, standard 95% extract is highly efficient. Because it is poorly absorbed, the majority of the active compound remains in the intestines, exerting its anti-inflammatory effects exactly where it is needed.
- For Systemic Inflammation: If you are trying to lower cardiovascular risks, address systemic joint issues, or support cognitive health, standard powders will offer little help. To shift systemic biomarkers like High-Sensitivity CRP (hs-CRP) or tracking liver function metrics, you must select an enhanced bioavailability curcumin format. Only these advanced delivery platforms ensure that the active curcuminoids survive digestion, escape liver clearance, and actively reach peripheral tissues.
Core Checklist for Choosing a Curcumin Supplement
When reviewing supplement labels or researching raw manufacturing ingredients for therapeutic applications, always look for these evidence-based markers of quality:
- [ ] Delivery Mechanism: Does the label explicitly mention a validated delivery system like a liposomal matrix, a phytosome, or a micellar system?
- [ ] Source Transparency: Ensure that the delivery components are derived from high-quality, stable sources, such as non-GMO sunflower lecithin rather than low-grade soy derivatives.
- [ ] Data Verification: Does the manufacturer provide clear, peer-reviewed human data showing actual improvements in serum concentration (ng/mL) rather than relying on ambiguous marketing buzzwords?
- [ ] Formula Intention: Match the supplement format to your health goals. Do not pay premium prices for lipid-based systems if you only want localized intestinal support, and do not buy standard powders expecting systemic changes.
Disclaimer: Always consult with a qualified healthcare provider before introducing new high-absorption supplement protocols, particularly if you are currently taking prescription blood thinners, diabetes medications, or undergoing active therapies that interact with liver clearance pathways.